Brief
An 18 year old girl is brought into ED resus. She was found on a park bench by a passer by with a bottle of Lambrini by her. Rouseable to a firm shoulder squeeze but behaving intoxicated with a strong smell of alcohol. Moving all 4 limbs and no signs of head injury. The pitstop nurse asks you to prescribe IV normal saline to sober the girl up faster.Questions
- How is alcohol excreted from the body?
- What order pharmacokinetics does alcohol exhibit?
- What then is the effect of giving IV fluids?
- What's wrong with the word arouseable?
Answers
How is alcohol excreted from the body?
To be precise there are many alcohols - here we are talking about ethanol. The vast majority of alcohol is metabolised, eventually ending up as carbon dioxide and water. A small amount comes out in the breath and and even smaller amount is renally excreted.
What order pharmacokinetics does alcohol exhibit
Alcohol is a drug that exhibits zero order pharmacokinetics (steady state of elimination). The reason for this is simply that the dose it is taken in is so huge that it saturates the enzymatic pathways for it's metabolism.
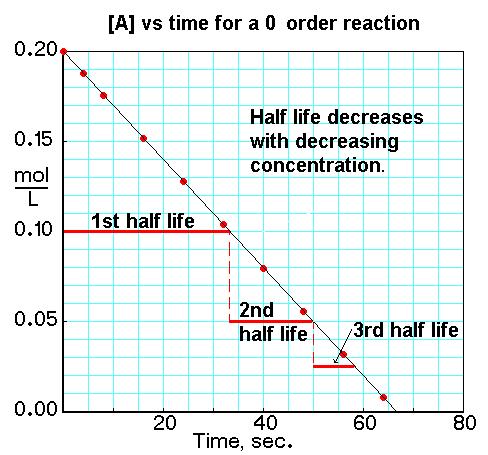 |
| Zero order pharmacokinetics |
What then is the effect of giving IV fluids
Theoretically giving fluids will increase the renal excretion of alcohol - but this only accounts for a small amount of the excretion. Both in laboratory and pragmatic studies this seems to give no benefit.
What's wrong with the word arouseable?
(From the Oxford English dictionary)
2Awaken (someone) from sleep:she had been aroused from deep slumberAlthough on ward rounds/in notes the use of 'arouse' where most people use 'rouse' can be the cause of great hilarity there is nothing wrong with it. It can also mean to excite sexually, but most people don't seem to take exception when I say "I'm going to turn on the lights." Sexual connotations are in the ears of the beholder.
